An 88 y.o. white male was admitted to Munson Medical Center in August 2006 with recurrent fevers and rigors.
A resident of Virginia the patient was visiting relatives in Traverse City when he abruptly became ill while attending a baseball game. Within a short time of his admission to the hospital he was found to be bacteremic with multiple cultures positive for Methicillin Resistant Staphylococcus aureus.
Previously, beginning in the spring of 2006, he had had a series of poorly explained bacteremic illnesses. These included Klebsiella bacteremia in March 2006, coincident Klebsiella and group A streptococcal bacteremias in May 2006, and coincident MRSA and Klebsiella bacteremias in June 2006. Workup including trans-esophageal echocardiography, WBC scan,
and abdominal and pelvic CT scans did not reveal an origin of his problem. Each time the patient was treated with courses of prolonged appropriate antibiotic therapy and appeared to improve.
The patient's past medical history was notable for coronary artery disease, peripheral vascular disease, and anemia that had previously required blood transfusion. In Aug 2000 he had undergone an Ancure aortic endograft repair of an infrarenal abdominal aortic aneurysm. Subsequent enlargement of the aneurysm was determined to be due to a Type 1 endoleak and necessitated open repair of the endograft in March 2002. He underwent colonoscopic polypectomy in the fall of 2005.
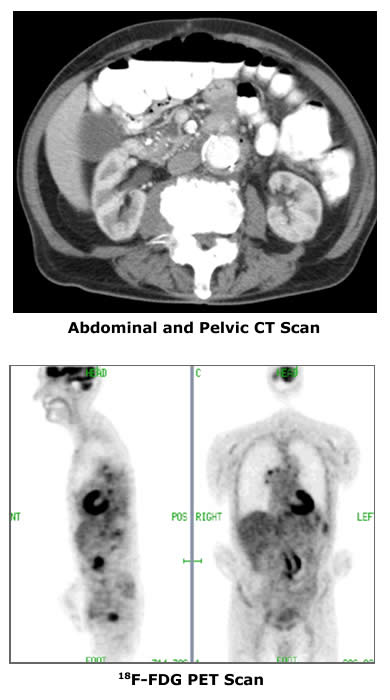
On examination the patient did not have focal localizing signs or symptoms. A systolic ejection murmur was noted. Initial laboratory data included WBC 21.4 (H) and Hgb 9.9 (L). LFT's and pancreatic enzymes were normal. An abdominal CT scan showed a 3.7 x 2.5 cm cystic mass in the head of the pancreas that may have been chronic. An additional image from that CT Scan is pictured at upper left. A trans-esophageal echocardiogram did not suggest the presence of valvular vegetations, and a labeled WBC scan was again negative (as it had been in Virginia).
The patient's bacteremia persisted for four days despite therapy with Vancomycin. He began to feel better only to suffer a relapse a week after admission at which time he was then found to be bacteremic with Klebsiella oxytoca.
Because the origin of the patient's bacteremias remained uncertain, a PET scan was performed. PET Scan images are pictured at lower left.
|