Infectious Diseases Case of the Month Case #1 |
|||
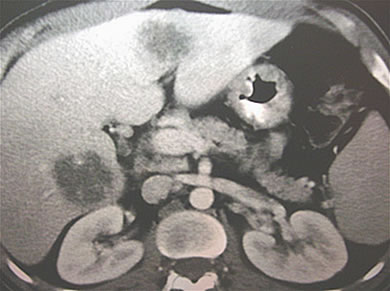 |
A 38 y.o. married hispanic male was admitted to the hospital with fever and RUQ pain. Though born in Mexico the patient had resided in north central Washington for the previous 18 years. For seven consecutive years he had worked on Alaska fishing boats in the summers. Recent catches were of hake and pollack. The boats he worked on were large with crews of multiple nationalities. Previously healthy, the patient became ill with fevers, nausea, vomiting and RUQ pain two days after his most recent fishing trip. He had no previous history of abdominal problems and had not had recent diarrhea. He denied substance use or history of STD or sexual promiscuity. Laboratory evaluation included: WBC 18.7 without abnormal eosinophilia; hgb 13.8; Bili 1.5; AST34; ALT 81; Alk Phos 291; amylase <30. His CT scan is pictured at left. |
||
What is your diagnosis? |
|||
|
These fairly well circumscribed hypodense lesions in the right and left lobes of the liver could certainly have multiple etiologies. Given the patient's ethnic background and exposure to fishing boat crew members of multiple nationalities, the possibility of amebic abscesses was early entertained as a likely diagnosis. He was begun on metronidazole and quickly experienced clinical improvement. Entamoeba histolytica serologies subsequently were positive (titer 1:1024). Serologies for Echinococcus were negative. The patient did not require drainage of the abscess, recovered uneventfully, and was treated subsequently with a course on an intra-luminal agent, iodoquinol. This man's case represents a somewhat typical presentation of persons with amebic liver abscesses. Clinical findings can vary but typically there is fever, right upper quadrant pain, and moderate leukocytosis. Intestinal symptoms may or may not precede the onset of specific signs and symptoms of liver disease. |
||
As in the case described, it is often unnecessary to drain amebic liver abscesses as they tend to respond well to medical therapy. Aspiration/drainage may be performed when an abscess is extremely large, when there is the potential for rupture, or when the diagnosis is in doubt. Complications of amebic liver abscesses include rupture across the diaphragm and resultant hepatobronchial fistula, pleural effusion and empyema, and lung abscess. Medical treatment is with a tissue active drug such as metronidazole followed by an intraluminal agent (referring to the gut lumen) to eliminate asymptomatic cyst carriage. Ref: Strickland, ed., Hunter's Tropical Medicine, 8th ed., 2000, pgs. 577-588. |
|||
| Home Case of the Month ID Case Archive | Your Comments/Feedback | ||